What Is Focused Ultrasound?
MRI-guided focused ultrasound (MRgFUS, or just FUS) focuses hundreds of ultrasound beams through the intact skull to a precise target deep in the brain to create a small, controlled lesion (disconnection) that interrupts the abnormal circuit driving your symptoms. There is no incision and no implanted device.
Precisely Targeted
Real-time MRI thermometry measures the temperature at the exact focus point, allowing the care team to confirm accuracy before the definitive treatment is delivered.
No Incision
The ultrasound beams pass through the skull without cutting. There is no opening in the scalp or skull, no implanted hardware, and no general anesthesia.
Awake & Interactive
You remain awake throughout so your care team can test symptom improvement in real time. Low-energy test pulses are given first so you can provide feedback before the permanent lesion is made.
Same-Day Discharge
Most patients are discharged the same day. Surgical recovery is typically quick and no follow-up for device programming (as for DBS) is needed.
How It Works — Step by Step
Surgery Without an Incision
MRgFUS is surgery because it achieves its effect by creating a permanent, targeted change in brain tissue. DBS, on the other hand, requires the surgical implantation of a device to deliver reversible, adjustable stimulation. Both are effective options; they work differently and suit different patients.
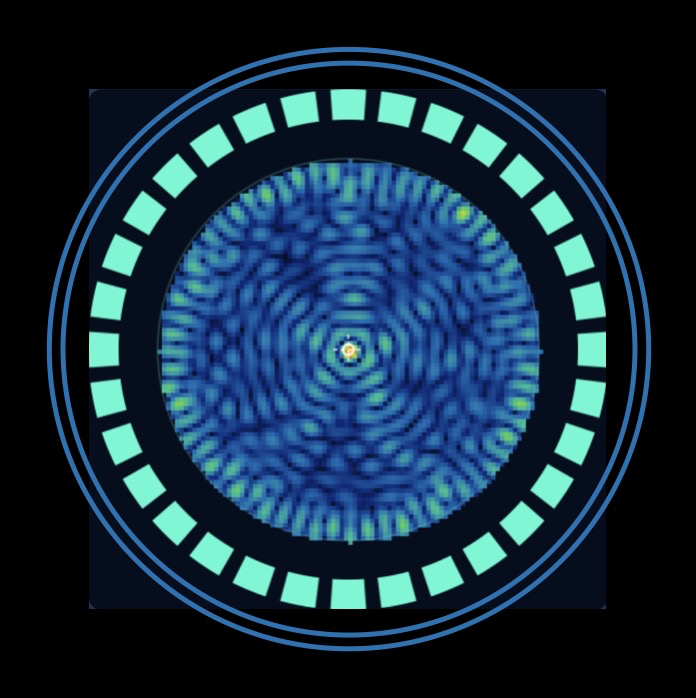
Ultrasound energy is delivered by individual "transducer" elements. Each transducer element on its own would spread energy across a wide volume of tissue. The waves of energy from each transducer will add or cancel, depending on their relative phases (where the peaks and troughs of the wave line up). The key is timing: when every element is delayed by exactly the right amount, all waves converge at the target simultaneously, arriving "in phase" and summing to produce an intensity far beyond what any single element could achieve.
Drag the target to steer the focus and watch each element's phase (shown by ring color) update in real time. Adjust the sliders to explore how the number of elements and phase accuracy (affected by skull density) shape the focal spot. Note that higher element counts are especially useful to correct for phase error, such as skull distortion.